What skin conditions are
Dermatosis is a broad term for changes that affect the skin and its appendages. It does not describe one single disease. It may refer to acne, melasma, rosacea, dermatitis, psoriasis, fungal infections, folliculitis, warts, hair loss, nail changes, stretch marks, scars, and lesions that may need biopsy.
The skin works as a barrier, an immune organ, a temperature regulator, and an interface with the environment. Sun, heat, humidity, cosmetics, medications, hormones, stress, genetics, infections, systemic diseases, and daily habits can influence symptoms such as itching, burning, pain, scaling, redness, spots, wounds, bumps, pustules, or hair loss.
Dermatologic treatment is not only about "erasing" a lesion. Good care seeks to confirm the diagnosis, reduce inflammation, control triggers, prevent scars, protect the skin barrier, recognize risk signs, and choose interventions compatible with age, pregnancy, breastfeeding, associated diseases, routine, skin phototype, and realistic expectations.




How dermatologic diagnosis is built
In dermatology, diagnosis is built from the combination of clinical history and skin examination. Lesion distribution, duration, itching, pain, burning, discharge, bleeding, scaling or fever, medication use, cosmetics, sunscreen, outdoor work, chemical exposure, and family history help guide the diagnostic hypothesis.
It also matters to know what has already been used. Corticosteroids, antibiotics, acids, lightening agents, antifungals, and ready-made mixtures can change how lesions look. In some cases, self-medication masks an infection, irritates the skin, worsens pigmentation, thins the skin, or delays diagnosis of conditions that need a specific approach.
The patient's report guides clinical reasoning: when it started, what worsens it, what improves it, which areas are affected, which products touch the skin, and how the condition affects sleep, work, self-esteem, and daily activities.
Direct observation evaluates color, borders, texture, elevation, scales, vessels, pustules, crusts, and distribution pattern. Dermoscopy magnifies details that are invisible to the naked eye and can be useful for moles, spots, hair loss, nails, and suspicious lesions.
Mycological scraping, culture, Wood's lamp examination, patch testing, laboratory tests, trichoscopy, or biopsy may be requested according to the clinical hypothesis. Not every case needs tests, but some depend on them for greater safety.
Treatment needs realistic goals, expected response time, correct use instructions, adverse-effect guidance, scheduled follow-up, and adjustments according to progress. Many skin conditions are chronic and controllable, not events solved by a single application.
Safety notice: local anesthesia, prophylaxis, lightening agents, antibiotics, isotretinoin, corticosteroids, antifungals, immunomodulators, biologics, and other medications require evaluation and prescription. Do not use them on your own or reuse old prescriptions without guidance.
Treatments: why there is no single recipe
Treatment for skin conditions may include proper cleansing, hydration, photoprotection, trigger control, topical medications, oral or injectable medications, procedures, dressings, and follow-up. The choice depends on diagnosis and severity. The same redness may be rosacea, dermatitis, lupus, allergy, fungal infection, or a drug reaction. The same spot may need simple care or further investigation.
In general, treatments are organized around four pillars: control the cause when it can be identified, reduce inflammation, restore the skin barrier, and prevent recurrence. In acne, for example, it is common to combine ingredients that unclog pores, reduce inflammation, and control bacteria; in melasma, photoprotection and control of pigment triggers are central; in psoriasis, immune modulation may be needed; in dermatitis, protecting the barrier and avoiding irritants is often decisive.
Creams, lotions, gels, ointments, and shampoos may contain retinoids, acids, antifungals, anti-inflammatory agents, therapeutic moisturizers, antibiotics, or lightening agents. Frequency and quantity matter as much as the product itself.
Oral or injectable medications may be indicated for severe acne, psoriasis, infections, urticaria, extensive dermatitis, and other diseases. They require assessment of contraindications, interactions, and sometimes monitoring tests.
Peels, lasers, light-based treatments, cryotherapy, injections, dermatologic surgery, and biopsy may be part of care, but they are not interchangeable. Indication depends on diagnosis, skin phototype, and risk of pigmentation or scarring.
Frequent skin conditions
Acne: follicle inflammation, scarring, and response time
Acne involves follicle obstruction, increased oiliness, proliferation of skin microbiota bacteria, and inflammation. It may appear in adolescence, persist, or begin in adulthood. In adult women, lesions on the chin and jawline, premenstrual worsening, and association with oiliness, hair loss, or menstrual irregularity may lead to hormonal evaluation when clinically appropriate.
Treatment may include gentle cleansing, non-comedogenic moisturizer, sunscreen, topical retinoids, benzoyl peroxide, azelaic acid, time-limited antibiotics, hormonal therapies in selected patients, isotretinoin for severe or resistant cases, and procedures for scars. Improvement is usually gradual; many guidelines recommend waiting several weeks to assess initial response, provided there is no major worsening or adverse effect.
For patients: squeezing lesions increases the risk of dark marks and scars. Harsh products, excessive exfoliation, and mixing active ingredients can irritate the skin and worsen the condition.
Melasma and dark spots: pigment, sun, and consistency
Melasma is an acquired hyperpigmentation, common on the face, influenced by ultraviolet radiation, visible light, genetic predisposition, hormones, pregnancy, contraceptives, and inflammation. Although it does not cause internal harm, it can affect self-esteem and quality of life. Control is usually long-term because skin prone to pigmentation reacts to repeated triggers.
The plan may combine broad-spectrum sunscreen, physical barriers, hats, sunglasses, tinted photoprotection, prescribed lightening agents, acids, antioxidants, tranexamic acid in selected cases, and procedures such as peels or lasers with great caution. Inappropriate treatment may irritate the skin, worsen pigmentation, or cause rebound.
Important: hydroquinone, retinoids, and other lightening agents should not be used without guidance, especially during pregnancy, breastfeeding, with sensitive skin, or in people with a history of irritation.

Rosacea: redness, sensitivity, and triggers
Rosacea is a chronic inflammatory condition that usually affects the central face. Flushing, persistent redness, visible vessels, burning, dryness, papules, and pustules may occur. Some people have ocular symptoms such as irritation, gritty sensation, red eyes, or inflamed eyelids.
Treatment may involve a gentle cleansing routine, barrier-repair moisturizer, photoprotection, trigger identification, topical medications such as metronidazole, azelaic acid, or ivermectin, anti-inflammatory-dose antibiotics when indicated, and technologies for visible vessels. Alcohol, heat, intense exercise, spicy foods, sun, stress, and irritating cosmetics may trigger flares in predisposed patients.
Attention: corticosteroid use on the face without follow-up may worsen rosacea, cause perioral dermatitis, thin the skin, and increase visible vessels.

Dermatitis: skin barrier, allergy, and irritation
Dermatitis is another broad term. It may be atopic, seborrheic, irritant, allergic contact, nummular, perioral, or related to medications and products. Itching, redness, scaling, fissures, and burning are common, but location and exposure history help differentiate the types.
Care may include barrier-repair moisturizers, reducing hot showers, gentle cleansers, removing irritants, time-limited anti-inflammatory treatment, and patch testing when allergy is suspected. In seborrheic dermatitis, oily areas such as the scalp, eyebrows, sides of the nose, and chest may scale, with skin microbiota participation and tendency to recur.

Psoriasis: inflammatory, chronic, and systemic disease
Psoriasis is an immune-mediated inflammatory disease, usually chronic, that can cause red, scaly plaques. It may affect the scalp, elbows, knees, nails, genital area, and folds. Some people have joint pain, swelling, or stiffness, which requires investigation for psoriatic arthritis.
Treatment options vary according to extent and impact: moisturizers, topical medications, phototherapy, conventional systemic medications, and biologic therapies in selected cases. Follow-up also considers comorbidities such as metabolic syndrome, obesity, smoking, mental health, and cardiovascular risk when relevant.
Seek evaluation: joint pain, morning stiffness, nail lifting, or extensive plaques deserve targeted discussion because they may change the treatment strategy.

Warts, moles, cysts, and non-healing lesions
Not every mole needs removal, and not every raised lesion is dangerous. Still, changes in color, size, shape, symptoms, or bleeding need evaluation. Non-healing wounds, recurrent crusts, painful lesions, moles that look very different from the others, or enlarging spots deserve attention.
Dermoscopy can help decide whether a lesion can be monitored, treated, removed, or biopsied. When surgical removal or biopsy is performed, the tissue may be sent for histopathology. This report is important to confirm diagnosis, margins, and whether additional care is needed.
Stretch marks, scars, and post-inflammatory dark marks
Stretch marks appear when dermal fibers partially rupture, which is common with rapid growth, pregnancy, weight gain, strength training, genetic predisposition, and inappropriate corticosteroid use. Recent stretch marks are often reddish or purple; over time, they may become whitish and more atrophic.
Treatments may aim to improve texture, color, and skin quality through topical ingredients, microneedling, lasers, radiofrequency, peels, or other technologies according to evaluation. The realistic goal is improvement, not a promise of total removal. In acne scars or post-inflammatory dark marks, the plan considers skin phototype, keloid tendency, scar depth, and activity of the underlying disease.

Biopsy de pele: quando pode ser indicada
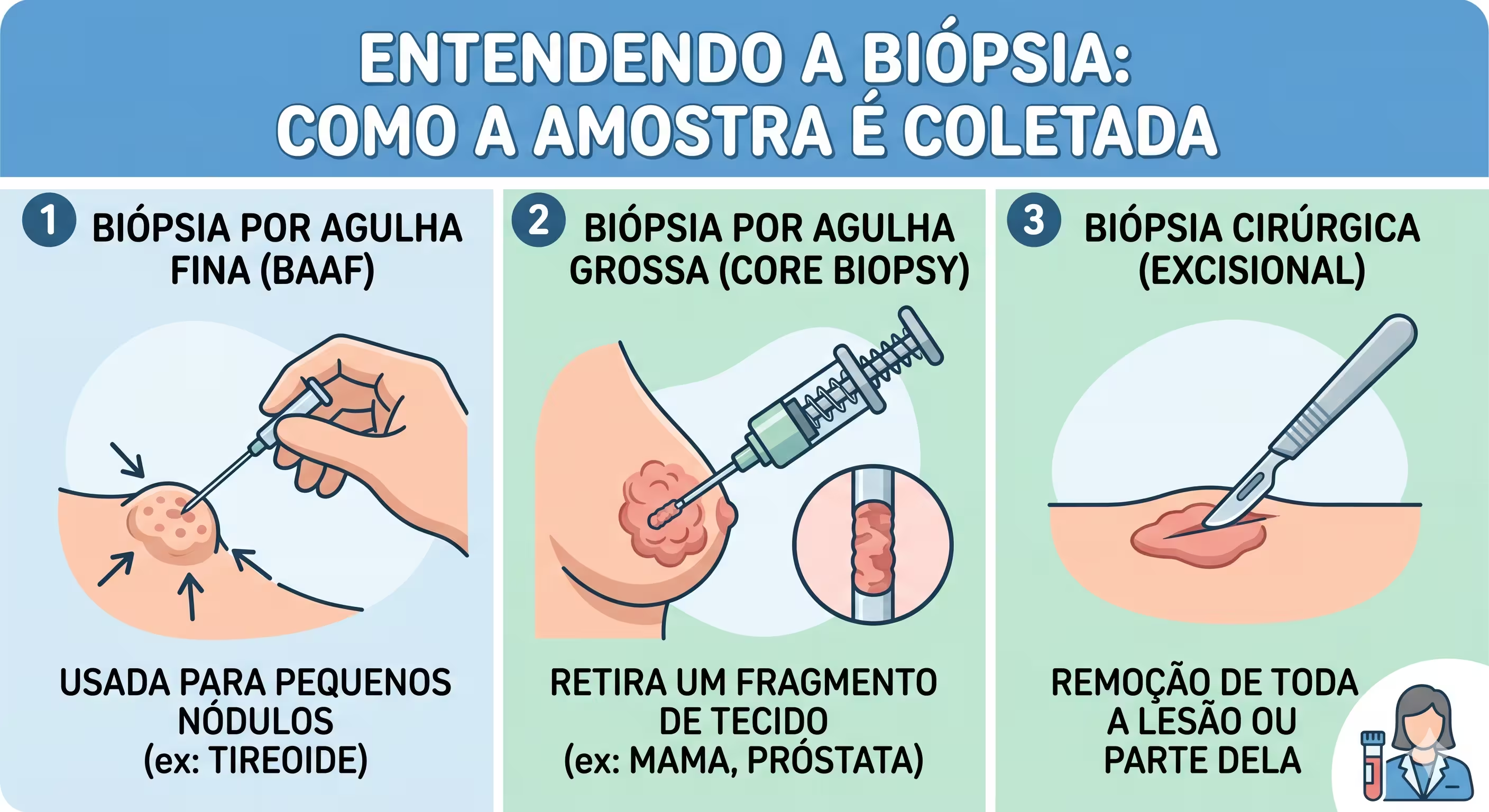
Biopsy is a procedure in which a small skin sample is removed for analysis. It may be indicated for suspicious lesions, persistent inflammation, blistering diseases, spots with uncertain diagnosis, scarring hair loss, non-healing wounds, or when microscopic examination can change treatment.
The biopsy type depends on the lesion: punch, shave, incisional, or excisional. The procedure is usually performed with local anesthesia when indicated and requires guidance about dressing care, bleeding, infection signs, suture removal, and follow-up. The decision must always consider risks, benefits, and diagnostic purpose.
When to seek dermatologic evaluation promptly
Some signs should not be managed only with internet research or over-the-counter products. They may indicate infection, drug reaction, significant inflammatory disease, precancerous change, or skin cancer. When in doubt, especially with rapid worsening, intense pain, or general symptoms, seek care.
- A mole or spot that changed size, color, border, elevation, sensitivity, or started bleeding.
- A wound that does not heal, a crust that keeps returning, or a persistent painful lesion.
- Extensive redness with fever, malaise, pain, local warmth, or discharge.
- Blisters or wounds in the mouth, eyes, or genitals, especially after starting a medication.
- Swelling of the face, lips, or eyelids, shortness of breath, or generalized hives.
- Rapid hair loss, scarred patches, pus on the scalp, or intense pain.
- Pregnancy, breastfeeding, immunosuppression, uncontrolled diabetes, or anticoagulant use before any procedure or new medication.
Home care that supports treatment
Daily care does not replace medications when they are necessary, but it can determine the success of the plan. Many skin conditions worsen when the skin barrier is irritated. Simple, sustainable, well-tolerated routines usually work better than product overload.
Photoprotection as a foundation of treatment
Sunscreen, clothing, hats, shade, and avoiding intense exposure are therapeutic measures for melasma, post-inflammatory dark marks, rosacea, cutaneous lupus, actinic aging, and skin cancer prevention. For facial pigmentation, tinted sunscreens may help block visible light, but the choice should consider sensitivity, oiliness, and patient adherence.
Gentle cleansing and the skin barrier
Very hot showers, harsh soaps, frequent exfoliation, and mixing acids may worsen dermatitis, rosacea, irritated acne, and itching. Regular hydration, cleansing suited to the skin type, and gradual introduction of active ingredients reduce abandonment and adverse effects.
Symptom tracking
Serial photos under similar lighting, a list of products used, symptom start date, foods or situations that preceded flares, and treatment responses help during the consultation. This record is especially useful for urticaria, rosacea, contact dermatitis, adult acne, and recurrent spots.


Consultation is the starting point for safe treatment
Bring your questions, products currently used, old prescriptions, tests, and progress photos. This helps turn scattered symptoms into a clear plan.
References and editorial criteria
This page was prepared as patient education material, based on technical content, medical safety review, and alignment with standards for medical advertising and health content.
The editorial criteria include educational language, professional identification, no promise of results, illustrative images, guidance toward individualized evaluation, reinforcement against self-medication, and prioritization of useful, reliable, people-first content.
- CFM Medical Advertising Manual and CFM Resolution No. 2.336/2023.
- Google Search Central: helpful, reliable, people-first content.
- Google Ads policies for healthcare and medicines.
Notice: terms such as anesthesia, prophylaxis, lightening agents, and medications involve prescription decisions and should not be used on your own.
Bibliographic references
- AMERICAN ACADEMY OF DERMATOLOGY ASSOCIATION. Acne: diagnosis and treatment. Rosemont: AAD, 2026. Available at: https://www.aad.org/public/diseases/acne/derm-treat/treat. Accessed on: June 17, 2026.
- AMERICAN ACADEMY OF DERMATOLOGY ASSOCIATION. Melasma: diagnosis and treatment. Rosemont: AAD, 2026. Available at: https://www.aad.org/public/diseases/a-z/melasma-treatment. Accessed on: June 17, 2026.
- AMERICAN ACADEMY OF DERMATOLOGY ASSOCIATION. Rosacea: diagnosis and treatment. Rosemont: AAD, 2026. Available at: https://www.aad.org/public/diseases/rosacea/treatment/diagnosis-treat. Accessed on: June 17, 2026.
- AMERICAN ACADEMY OF DERMATOLOGY ASSOCIATION. How dermatologists diagnose and treat psoriasis. Rosemont: AAD, 2026. Available at: https://www.aad.org/public/diseases/psoriasis/treatment. Accessed on: June 17, 2026.
- AMERICAN ACADEMY OF DERMATOLOGY ASSOCIATION. Find skin cancer: how to perform a skin self-exam. Rosemont: AAD, 2026. Available at: https://www.aad.org/public/diseases/skin-cancer/find/check-skin. Accessed on: June 17, 2026.
- NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Acne vulgaris: management. NICE guideline NG198. London: NICE, 2021. Atualizado em: 30 abr. 2026. Available at: https://www.nice.org.uk/guidance/ng198. Accessed on: June 17, 2026.
- FEDERAL COUNCIL OF MEDICINE. Medical Advertising Manual: CFM Resolution No. 2.336/2023. Brasilia, DF: CFM, 2024. Available at: https://publicidademedica.cfm.org.br/. Accessed on: June 17, 2026.
- GOOGLE. Creating helpful, reliable, people-first content. Google Search Central, 2026. Available at: https://developers.google.com/search/docs/fundamentals/creating-helpful-content. Accessed on: June 17, 2026.
- GOOGLE. Healthcare and medicines: Google Ads policies. Google Ads Policies Help, 2026. Available at: https://support.google.com/adspolicy/answer/176031. Accessed on: June 17, 2026.
- BOLOGNIA, Jean L.; SCHAFFER, Julie V.; CERRONI, Lorenzo. Dermatology. 5. ed. Philadelphia: Elsevier, 2024.